There has been a lot of talk about TIR (Time in Range) and SD (Standard Deviation) being more useful measures of glycaemia than HbA1c. Looking back at my own experience I can see an issue relevant to this.
I should reiterate:
HbA1c only indicates what your average BG was.
It says nothing about how wild a rollercoaster you’ve been on (with a high SD value) and whether you were having daily dangerous hypos.
Or whether you’d managed to keep things around your average level all day (with a low SD).
But HbA1c is entrenched for a few reasons, such as:
- It can be measured via a blood test without having to equip the person with CGM technology.
- We have lots of HbA1c records from the past to compare with.
- Many clinical trials have used HbA1c as a primary end-point to measure the effectiveness of a treatment. And while we know that HbA1c is not a good measure by itself, this still happens even today as new trials compare their data with those of previous publications. It’s a Catch-22 feedback loop.
- Some doctors seem stuck in their ways.
HbA1c is no longer held up as a measure to gauge your eligibility to hold a driving licence (this was clarified in 2016). However HbA1c is still a measure that many doctors and patients refer to.
I still see people saying they’re trying to get their HbA1c down. As someone who tried that in the past, maybe my experience will be useful.
To achieve a lower HbA1c, I would not aim to get a lower HbA1c.
Wait, what?
The wrong target to concentrate on
Achieving a lower HbA1c is not necessarily a bad thing, but it’s better as an outcome than a specific thing to concentrate on achieving.
Aiming for a lower HbA1c means you will be aiming for a lower BG average. And as such you’re concentrating on things like bolusing more insulin for higher levels. Obviously you’re trying to balance that against the risks of too-low BGs and hypoglycaemia, but your mental target is usually to “beat down” those highs.
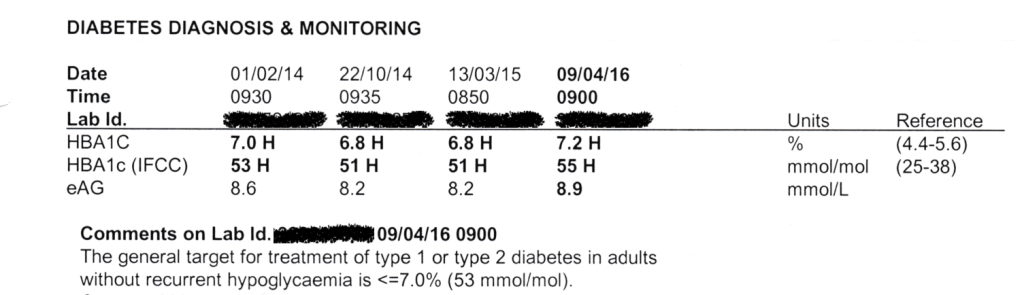
In 2016 my HbA1c was 7.2% and although some people will see that as aspirational, I decided I wanted to get it down. And after months of intensive management using many corrections on my pump, I did get it down. I got it to 5.9%. But not safely.
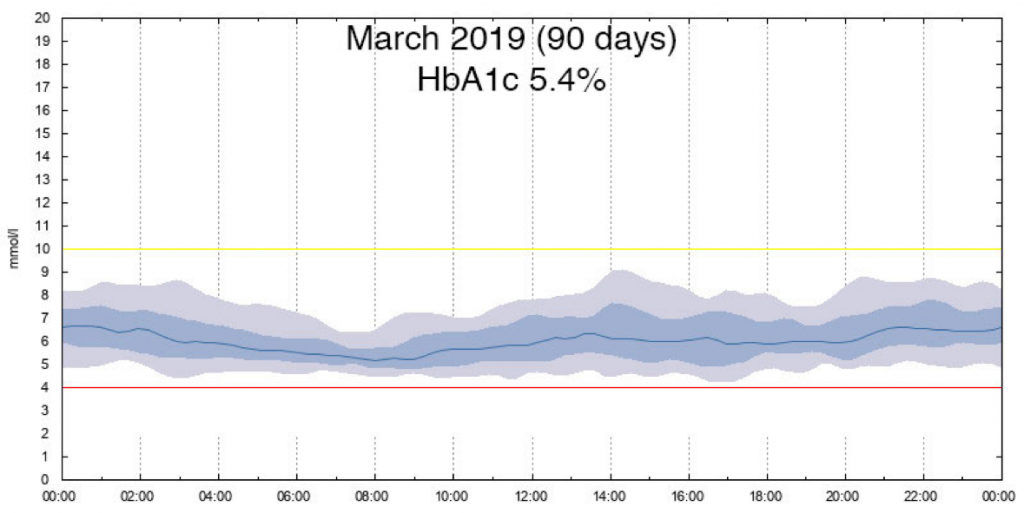
I was using Libre at the time, although I wasn’t using the CGM data as effectively as I do today. Looking back through the historical data we can see what was happening. This is where I started:
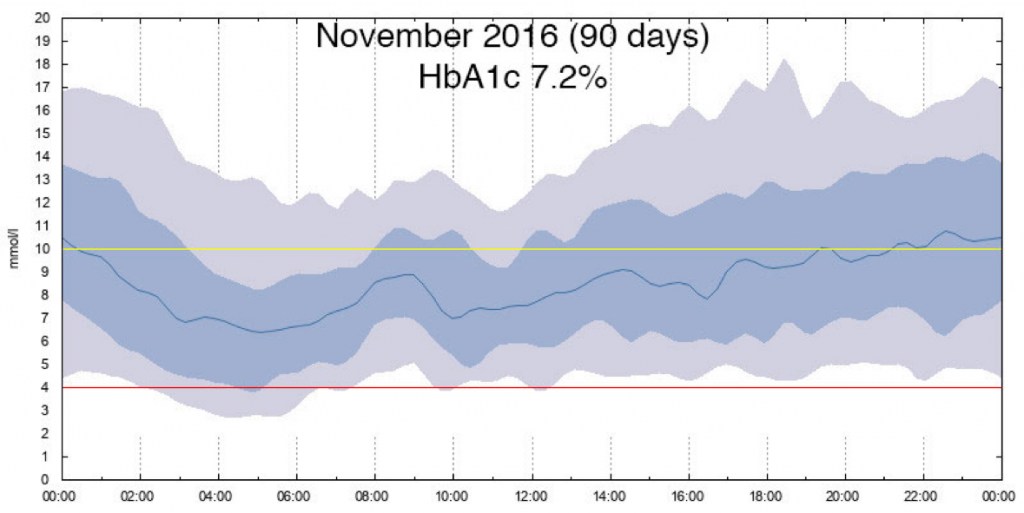
This is an “AGP” or “Percentile” chart, with all the 90 daily traces laid over each other and blended. The dark line in the middle is the average for that time of day. The blue band in the middle contains 50% of the readings (from the 25th to 75th percentile) and the lighter bands outside that mark the 10th and 90th percentiles. It’s only the average of all those numbers which equates to the HbA1c result.
Looking back at that data, I remember I was conscious of all those readings up in the high teens, and wanted to get rid of those. Obviously there was also an overnight hypo problem at least 25% of the time, but having grown up using basal insulins like Monotard and Lantus, I guess I was used to that and didn’t see it as a bigger problem than the highs. Also I and my doctor did not have this AGP graph to review at the time.
So after a few months of intensive self-management trying to keep my BG down around 5.5 mmol/l, I got my HbA1c down to 5.9%!
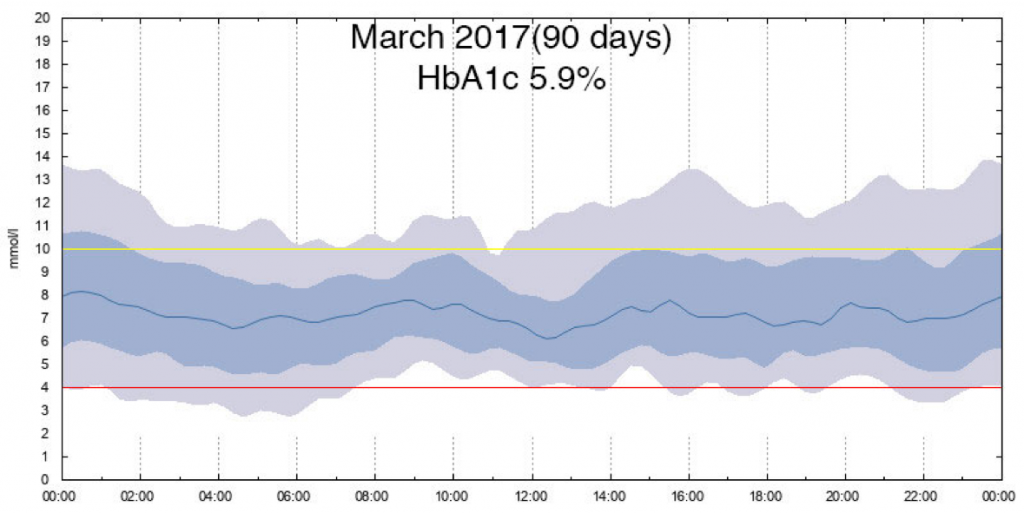
As you can see, I had indeed managed to reduce a lot of those highs and narrow the spread a lot. But now I had a lot of hypo issues throughout the day. Do note that none of these hypos were debilitating: I was always able to snack my own way out of a hypo.
Quite understandably my endo was concerned about all those hypos. Not only was the 5.9% lower than he was expecting, we did have this graph to look at. We changed a bunch of things and my next result was 6.5% (with that graph basically shifted up slightly). Incidentally, up until this point I’d been using an Animas Vibe pump with manual corrections.
But I knew from the experiences of other people using CGM that it was possible to have an HbA1c below 6% and be safe. I just hadn’t managed it well. So I tried a different approach.
Trying to “stay in range” is safer and more effective
As I described in my “Targets and Goals” article, I started off by having my goal as the standard clinical range of 3.9-10 mmol/l, with 5.5 mmol/l as the target for any corrections.
When my BG was going to head above 10 (or maybe already had) I applied corrections to get me down, but if it only came down to 8.0 I wouldn’t aggressively keep bolusing to get it to the “optimal” 5.5 mmol/l. Yes I would eventually get it back to target, but as long as it was between 3.9-10 I was happy.
At the same time I did my best to keep my BG above the bottom goal: 3.9 mmol/l.
This is not the same as telling my pump’s bolus wizard to use 3.9-10 as a target. If I did that, a correction bolus would only be trying to get me down below 10 (and stay above 3.9). I told my pump to aim at 5.5, although it would rarely get there on its first try and I was OK with that.
In a football analogy: I was aiming at a particular target within the goals, but as long as the ball went between the goal posts I was happy.
I learnt not to let it run too close to the goal posts for long periods in order to not have it drift out while I wasn’t looking.
One way of talking about what I was doing: I was increasing my Time in Range.
So what happened?
An even-lower HbA1c number!
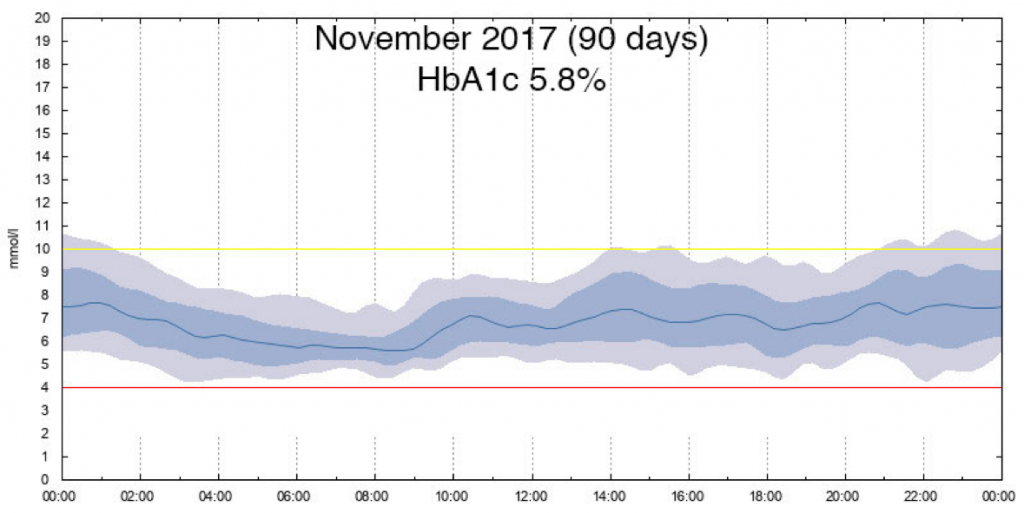
You can see there that my BG still didn’t stay within the range 100% of the time (remember there’s 10% above and 10% below that grey band). But it was inside most of the time, and in fact it spent most time well within range.
Obviously this was working (and my endo was happy with this result even though the HbA1c was lower than that earlier “bad” 5.9%) so I kept going! As mentioned in Targets and Goals, after I’d increased my TIR for 3.9-10 further I later narrowed my goal range (with my CGM showing me the feedback of a different colour number when it went above range, but not disturbing my life with alarms until it hit 12 mmol/l) to 3.9-9. And then when I was managing a high TIR for that range, I narrowed again to 3.9-8. Later I settled on 3.9-7.8, which I’m still using today.
I haven’t lowered the bottom end of the range, but bringing the top end down has moved the average down at the same time.
In terms of TIR for the standard clinical range of 3.9-10 mmol/l, back in 2016 with that 7.2% HbA1c I was only in range 53% of the time. Today I average over 95% (less for the 3.9-7.8 range I use, but aiming at the tighter range automatically means more levels will fall within 3.9-10).
Now I am using a closed-loop pump/CGM system to help me achieve this, but the mental approach along the way has always remained the same.
At no point have I said “I want to get an HbA1c below 5.5%”.
I’ve just tried to increase the time I spend between my goal posts.
And lower HbA1c numbers have just turned up on the blood test results!
My advice
It may sound contradictory, but if you’re hoping to get a lower HbA1c number (even if it’s not as low as I’ve shown here) I would advise Don’t aim at lower numbers! Aim at more-controlled numbers.
That’s as close to “medical advice” as I should go, but hopefully that message can be applied usefully in your own management (which you can discuss with your medical team). As you can see, it’s worked for me. That doesn’t mean it will necessarily work for everyone of course (“Your Diabetes May Vary”) but I think it’s worth considering.
Having CGM technology is a massively-useful advantage in this management, but the same thing can apply to results from fingerprick BG readings.
Very interesting. What did you actually do to get such a flat line throughout the day? Are you eating smaller carb portions? This seems to be the only thing I can see to do to avoid spiking up to 12+ after certain meals — e.g. breakfast which is often higher carb and more easily absorbed carbs.
Yes I am being very conscious of my carb intake, and tend to avoid “spiky” foods. But I’m not “low carb” per se.
Overall my diet has been around 250-350 g of carbs per day (adding up the records from pump in review: again that’s not a target I count my way towards).
Having my basal rate tuned so it will keep me flat in the absence of food is important, as that allows the corrections on top of that to do what they’re supposed to.
After that it’s a matter of choosing sensible foods, getting the bolus doses right, and getting the timing of doses right.
Mind you, having a closed-loop system making pump adjustments every 5 minutes in the background based on the CGM data doesn’t hurt…
Great article as always!
You’ve done well to preserve your data so well over the years
I read Dr Bernstein book and did a no or very low carb diet. My HBA1C went down from 7.2% to 5.8%. with many hypos. Both my Endo and my CDE said that was to low especially for older type 1s. Was trying to reduce my HBA1C so to reduce complications. Both of my health professionals said the the average BG was more important. now I am not so fixated and I am living better even though my HBA1C has gone up according to CareLink.If you can believe it.
Can I ask, did you do any basal testing? Basal seems to be the key but it’s the trickiest thing for me…
Back in early 2017 with the Vibe? Not really as a separate exercise, but we did get the basals a lot closer to right than they had been.
Thank you for sharing your experience! Do you think it’s possible to achieve such a good result (as in your last picture) without a closed-loop system?
Possible, I’m sure yes. But I wilt at the thought of how much constant attention it would require.